



The Oxford Partial Knee Replacement: The Normal Feeling Knee Replacement
Aug 22, 2019Richard A. Sweet, M.D. (Retired 2022)
Introduction: Full vs. Partial Knee Replacement
Each year hundreds of thousands of Americans with painful arthritic knees face the prospect of undergoing traditional full knee replacement surgery. Though highly successful at relieving the pain and disability of arthritis, patients observe that the new knee does not feel “normal”. This is largely due to the fact that in full knee replacement surgery the anterior cruciate ligament (ACL) is sacrificed. The result is that the artificial knee does not have the same stability and kinematics as does a normal knee. However some patients, depending on the type and location of the arthritic disease, do have an alternative option. This option is the partial knee replacement. The partial knee replacement’s major advantage over the traditional full knee replacement is that all four of the major ligaments of the knee, including the ACL, are preserved.
Anatomy of the Arthritic Knee
Knee Compartments
There are 3 compartments of the knee, each of which can be involved in the arthritic process:
- The medial (inside) compartment of the knee. When arthritis is isolated to the medial compartment a patient is a candidate for a partial knee replacement.
- The lateral (outside) compartment of the knee. When arthritis involves the lateral com-partment of the knee, a partial knee replace-ment is contraindicated. In this situation, a full tri-compartmental replacement is required.
- The patella-femoral (knee cap) compartment. A partial knee replacement can still be considered in the presence of mild patella-femoral arthritis. If the arthritis is more severe, a complete replacement is required to obtain satisfactory pain relief.
Knee Ligaments
In the normal knee there are 4 major stabilizing ligaments. These include:
- The medial and lateral collateral ligaments (MCL & LCL) are located on the inside (medial) and outside (lateral) part of the knee. They control side-to-side knee stability. Both the MCL and LCL are routinely preserved in all knee replacement surgery.
- The posterior cruciate ligament (PCL) is located in the center-back of the knee. It controls posterior knee stability. In the full knee replace-ment surgery it’s usually preserved, though in certain circumstances it can be substituted for.
- The anterior cruciate ligament (ACL) is located in the center-front of the knee. It controls anterior and rotational knee stability. It is sacrificed in all traditional full knee replacement designs. It is, however, preserved in partial knee replacement procedures.
Partial Knee Replacement Indications
Indications for partial knee replacement surgery include:
- Medial Compartment Arthritis: The major indication for partial knee replacement surgery is significant arthritis isolated to the medial compartment of the knee. A mild amount of patellar arthritis is tolerable.
- Intact ACL: The ACL must be functional for the procedure to succeed.
Advantages of the Partial Knee Replacement:
The 3 major advantages of partial knee replacement surgery include:
- Bone and Cartilage Sparing: The normal lateral and patella-femoral compartments of the knee are preserved.
- Minimally Invasive: By avoiding cutting of the quadriceps muscle, the operation is “minimally invasive” thus leading to faster recovery and quicker rehabilitation resulting in a more rapid return to full activity.
- Anterior Cruciate Ligament (ACL) Preservation: The major advantage of partial knee replacement is the preservation of the anterior cruciate ligament, which is routinely sacrificed in traditional full knee replacement procedures. Because of this, partial knee replacement patients typically find their new joint feels much more like the normal knee.
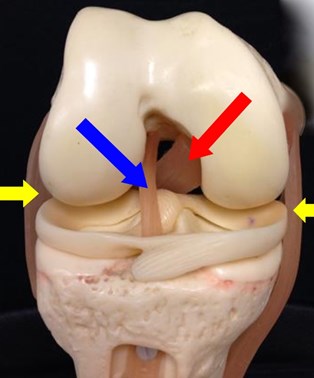 Figure 1: The arrows indicate the 4 major ligaments of the knee. Yellow – medial and lateral collateral ligaments. Red – Posterior Cruciate Ligament. Blue – ACL
Figure 1: The arrows indicate the 4 major ligaments of the knee. Yellow – medial and lateral collateral ligaments. Red – Posterior Cruciate Ligament. Blue – ACL Figure 2: The Oxford partial knee replacement preserves the ACL.
Figure 2: The Oxford partial knee replacement preserves the ACL.Risks of Partial Knee Replacement
There are inherent risks unique to partial knee replacement surgery relative to the traditional full tri-compartmental replacement that can lead to the need for further surgery in the future.
- Implant Loosening: The components of the partial knee replacement are much smaller than those of the full knee replacement. With a smaller surface for which the cement to gain purchase, early implant loosening in the first few years post op can, in a small percentage of patients, occur. When cement loosening occurs, further surgery to convert to a full tri-compartmental replacement is required.
- Arthritis in the Un-Replaced Knee Compartments: Occasionally arthritis will progress in the un-replaced lateral or patella-femoral compartments of the knee. This can lead to the need to convert to a full knee replacement.
The Oxford Partial Knee Replacement
The Oxford Partial Knee Replacement was developed over 2 decades ago by surgeons in the United Kingdom. It was approved for use in the USA in 2004. It is a “mobile bearing” design where the plastic “cushion” can float freely on the tibia baseplate while articulating with the femoral component above. This unique design decreases the stress on the underlying cement and the plastic lowering the risks of cement loosening and plastic wear.
 Figure 3: This knee x-ray shows bone on bone arthritis isolated to the inside medial part of the knee.
Figure 3: This knee x-ray shows bone on bone arthritis isolated to the inside medial part of the knee. Figure 4: This medial compartment that has undergone a partial Oxford knee replacement. The outside lateral compartment and patella-femoral compartment are preserved.
Figure 4: This medial compartment that has undergone a partial Oxford knee replacement. The outside lateral compartment and patella-femoral compartment are preserved.




 Our patients can receive MRI imaging onsite at both our Louisville and New Albany Clinics.
Our patients can receive MRI imaging onsite at both our Louisville and New Albany Clinics. Providing the latest advances in orthopedic surgery is our specialty.
Providing the latest advances in orthopedic surgery is our specialty. We take a unique, multidisciplinary approach to pain management.
We take a unique, multidisciplinary approach to pain management. Our physical therapists use advanced techniques to help restore strength and mobility.
Our physical therapists use advanced techniques to help restore strength and mobility.  We provide comprehensive, conservative care for a wide variety of foot and ankle conditions.
We provide comprehensive, conservative care for a wide variety of foot and ankle conditions. We offer same- and next-day care to patients with acute injuries.
We offer same- and next-day care to patients with acute injuries. Get back in the game with help from our sports medicine specialists.
Get back in the game with help from our sports medicine specialists.  Our centers are equipped with a state-of-the-art digital X-ray machine.
Our centers are equipped with a state-of-the-art digital X-ray machine.