



Lumbar Disc Herniation
Aug 22, 2019A Comparison of the Results of Chemonucleoysis and Open Disectomy After Ten Years
Abstract:
Using data obtained by questionnaire in a retrospective review of pati ents with low-back and sciatic pain (eighty-five treated by injection of chymopapain and seventy-one, by open discectomy), the results at one and ten years after treatment were analyzed. For this analysis we used six measures of pain relief, six measures of the patients’ course during the ten-year pe-riod since primary treatment, and four measures of the patients’ history of employment or work since initial treatment. Valid ity studies demonstrated that the pain-outcome measures reflected the patients’ condition ade-quately and that all six measures were significantly re-lated to each other (Pearson’s r, p < 0.003). The chymopapain and discectomy were not distin-groups guishable on the basis of the tcome measures.pain-ou However, body mass was directly related to the presence of pain ten years after discectomy but not after injection of chymopapain.
Analysis of the progress measures (indicators of the course of the patients’ pain during the ten-year period) showed that the rates of reoperation in the two treatment groups did not differ significantly, but the discectomy patients tended to have had a higher rate of reoperation at both one and ten years after initial treatment. These measures did not show unequivocal superiority of one treatment compared with the other.
Using the work measures (assessments of the patients’ history of employment since initial treatment), it was found that in both treatment groups the patients who returned to work six to twelve weeks after treatment despite persistent symptoms had significantly more pain at ten years (p < 0.04). Also, the patients who returned to work less than six weeks after treatment, while still symptomatic, showed a similar trend. On the other hand, among the patients who were still symptomatic at twelve weeks, it made no difference in the final results whether they returned to work at twelve weeks or there-after. These findings support the notion that after either discectomy or chemonucleolysis, patients should return to work only after complete symptomatic recovery or a minimum convalescence of twelve weeks.
It has been fifty years since Mixter and Barr first operated on a patient for a herniated nucleus pulposus and twenty years since Smith first injected chymopapain into the nucleus pulpous of humans. Today, disagreement as the the efficacy of these two treatments continues. It is generally agreed that for most patients with lumbar or lumbosacral herniation, conservative treatment is preferable initially. Then, if recovery is delayed after such treatment, surgical intervention in the form of open discectomy or of percutaneous injection of chymopapain may be considered.
Indications for each of these techniques vary according to personal opinion. The potential advantages and disad-vantages of each procedure have been discussed12, but the indications for chymopapain as opposed to open surgery in the treatment of disc prolapse remain unsettled. Although some authors have reported comparable results with the two methods”, others have reported less favorable results with chymopapain4.1 1.2] . In addition, when they compared the outcomes of operative and conservative therapy in selected patients five, ten, and twenty years after treatment, Hake-lius, Weber, and Nashold and Hrubec did not find any significant differences between the final results of surgical and non-surgical treatment.
Although there have been numerous reports on the results of treatment of patients with sciatic and low-back pain 3,4,6-8,10.12,14-16.20.22 no studies have compared the long-term effects of chymopapain with those of laminectomy and discectomy in the treatment of a herniated disc. Some au-thors have reported more favorable results in patients who were treated by laminectomy, but doubt remains about whether surgical treatment has any advantage over chy-mopapain or conservative treatment in the long run 6,12,15,22.
The purpose of our study was to compare the results of treatment of lumbar and lumbosacral disc herniations by chymopapain injection and by discectomy after ten years. The patients so treated were compared with respect to their general well-being (outcome measures) after ten years and with respect to their course (progress measures) during the ten-year period. The outcome measures included indices of pain and disability at ten years, while the progress measures included speed of relief of symptoms, duration of relief, rate of reoperation after a successful initial procedure, and satisfaction with treatment. It was hypothesized that after ten years no major differences between the chymopapain and discectomy groups would be found based on the out-come measures. However, it was expected that chymopapain patients and discectomy patients would differ in terms of some of the progress measures. Thus, it was anticipated that chymopapain patients would report more rapid relief of symptoms, longer relief from symptoms, and lower rates of reoperation than would the discectomy patients. A second area of interest was the relationship between type of treat-ment and capacity to work. This relationship was explored using work measures, but no specific hypotheses were pro-posed.
Study Population
The study population was composed of two groups. One group comprised patients who were treated by chy-mopapain injection by one of three orthopaedic surgeons at the Rush Presbyterian-St. Luke’s Medical Center in Chi-cago, Illinois. These patients came from across the conti-nental United States because they were part of an experimental protocol in Illinois that was developed by Bax-ter-Travenol and approved by the Food and Drug Admin-istration. Uniform records were kept on these patients using the Baxter-Travenol protocol. The other group was com-posed of patients who were treated by open discectomy performed by one of four spine surgeons at the University of Iowa Hospitals and Clinics in Iowa City, Iowa. Most of these patients were from Iowa. Standard hospital records were kept on these patients.
The criteria for inclusion in this study were: limited straight-leg raising on the affected side; reflex changes on the affected side; motor or sensory changes, or both; a minimum period of conservative treatment of three months; a positive myelogram, consistent with the history and phys-ical findings; and a minimum follow-up of ten years after original treatment. Patients who had had surgery on the lumbar spine or chemonucleolysis before the procedure that was to be studied, or had had a specific spinal lesion, in-cluding infection, tumor, spondylolysis, or spondylolis-thesis, were excluded. Patients with generalized arthropathy or a diagnosed neurological disorder, including a cauda equina syndrome and bladder dysfunction, were also ex-cluded.
On the basis of these criteria, 156 chymopapain patients and 100 discectomy patients were identified as satisfactory for inclusion. All available means were used to locate these 256 patients: state and local government agencies were con-tacted, telephone calls were made, and letters were sent. Twelve of the chymopapain and nine of the discectomy patients had died, and fifty-six (36 per cent) of the chy-mopapain and twenty (22 per cent) of the discectomy pa-tients could not be located. Of the remaining eighty-eight chymopapain patients who were reached, eighty-five (97 per cent) responded, while all of the seventy-one discectomy patients who were located responded.
In the chymopapain group the patients had been in-jected in the lateral decubitus position, while in the discec-tomy group a standard posterior midline approach to the lumbar spine had been used. The surgical group was some-what heterogeneous in that either a hemilateral or a bilateral laminotomy or even a bilateral laminectomy had been per-formed when indicated.
Instrumentation
The questionnaire used in this study was designed to provide measures of three distinct yet related aspects of the patient’s condition since treatment: pain-outcome measures – indicators of the patient’s condition or state of well-being ten years after treatment, progress measures – indicators of the status of the patient’s back during the ten-year period, and work measures -a special classification of the progress measures that reflected the patient’s occupational history during the ten-year period.
The questionnaire included questions that were relevant to all three measures. For the pain-outcome measures, six well accepted measurements were used: Pain Thermometer, Pain Status, Average Pain 1, Average Pain 2, Visual An-alogue Scale, and Disability Questionnaire.
The Pain Thermometer17,18 was an illustration showing a six-point scale resembling a thermometer. On the illus-tration, patients were asked to rate their pain at the time of receipt of the questionnaire. The scale ranged from one (no pain at all) to six (the pain is almost unbearable).
Pain S tatus5.9-1 was a five-point scale on which the patients rated any change in pain status during the previous year. This scale ranged from one (excellent, no pain) to five (worse than in prior years).
Average Pain 1 and Average Pain 25,9-11 were additional ratings based on questions that asked the patients to rate their pain from zero (no pain at all) to 100 (the most severe pain imaginable). Average Pain 1 was the patients’ rating of their average pain during the past ten years and Average Pain 2 was the patients’ rating of their average pain during the past few days before participating in this study.
The Visual Analogue Scale5.9-11 was a fifteen-item scale, with each item designed to assess the severity of the patients’ pain and symptoms. Each item included a state-ment concerning pain or symptoms accompanied by an an-alogue scale (a line of fixed length with extreme response possibilities at the two ends, the positive and negative anchor points). For each item, patients were asked to place an x somewhere on the scale at the point that best reflected their condition with respect to that item. For example, for the question “How severe is your back pain?“, the positive anchor point of the scale was “no pain” and the negative anchor point was “intolerable pain’ ’ . For each of the fifteen items, the distance from the positive anchor point to the x mark was measured, and then the fifteen distances were standardized so that the mean was zero and the standard deviation was one. The total score was then determined by summing the fifteen positive and negative scores. Thus, a total score that was a positive number represented a greater than average and a negative number, a less than average pain score.
The Disability Questionnaire13 was a scale based on twenty-four true-or-false items that were designed to assess the patients’ pain, symptoms, disabilities, or attitudes con-cerning their condition. Items were scored so that a one was awarded for responses that implied greater disability and a zero was awarded for responses that implied lesser disability. Thus, larger scores implied greater pain or disability.
For the determination of the progress measures, ques-tions were asked concerning the relief of pain after the original procedure; recurrence of pain, if any; and the need for additional treatment, including subsequent operations (defined as any open procedure on a patient who was initially treated with chymopapain or as another surgical procedure on a patient who was initially treated by discectomy). The indications for such additional treatment were recurrent sub-jective symptoms or objective findings associated with back pain or lower-extremity pain, or both, that had not responded to conservative treatment.
Based on the answers to these questions, six progress measures were developed as variables, and these variables each were divided into two to five categories to which the patients were asssigned on the basis of their symptoms as shown in Table V. The six variables were speed of recovery, which was the time required for symptomatic relif to occur after the primary treatment and included five categories ranging from no recovery to immediate recovery; duration of recovery, which was the duration of symptomatic relief after primary treatment and included four categories ranging from 0.5 to one year to seven years or more; duration of pain before additional treatment was sought, which included three categories – zero to two years, two to six years, and seven years or more; number of episodes of back pain per year since primary treatment, which had three categories -zero to four episodes, five to fourteen, and fifteen episodes or more; rate of recurrence after primary treatment, which was the number of patients who had had some additional treatment at one year and at ten years after primary treatment and included two categories – additional treatment within the first year and additional treatment by the ten-year follow-up; and number of hospitalizations for back pain after pri-mary treatment, a dichotomous variable that was recorded as either no or one hospitalization or as more than one hospitalization.
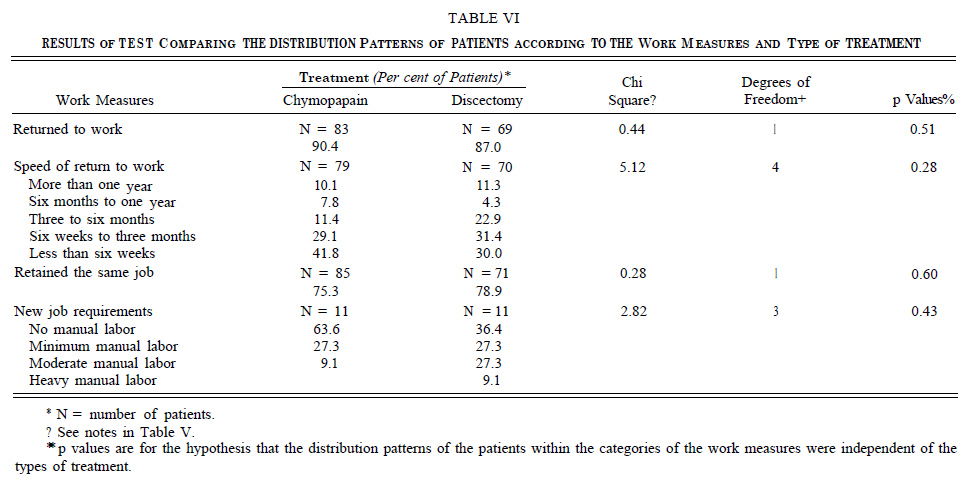
To determine the work measures, questions were asked concerning whether the patients had returned to work, the time of return to work, and any changes in their job or in the level of activity required for their current job. Based on the answers to these questions, four work measures were developed as variables (Table VI) which, like the progress measures, were divided into categories as follows: returned to work, a dichotomous variable that was rated as either one (yes) or two (no); speed of return to work, which was the length of time after primary treatment before returning to work and was divided into five categories ranging from more than a year to less than six weeks; retained the same job, a dichotomous variable that was rated as either one (yes) or two (no); and new job requirements, which was the level of manual labor required for the patients’ current job and had four categories that ranged from no manual labor to heavy manual labor.
In addition to developing the pain-outcome, progress, and work measures, we also attempted to assess the effects of the time of returning to work on the result. To do this, three composite variables (A, B, and C) were developed. These were based on the time after treatment when the symptoms were relieved (a progress measure) and the time when the patients returned to work (a work measure). Using these composite variables, the patients were divided into three composite-variable groups and the patients in each of these groups were subdivided according to the time of relief of symptoms and the time of return to work. The corre-sponding composite-variable subgroups in the chymopapain and discectomy groups were then compared.
Results
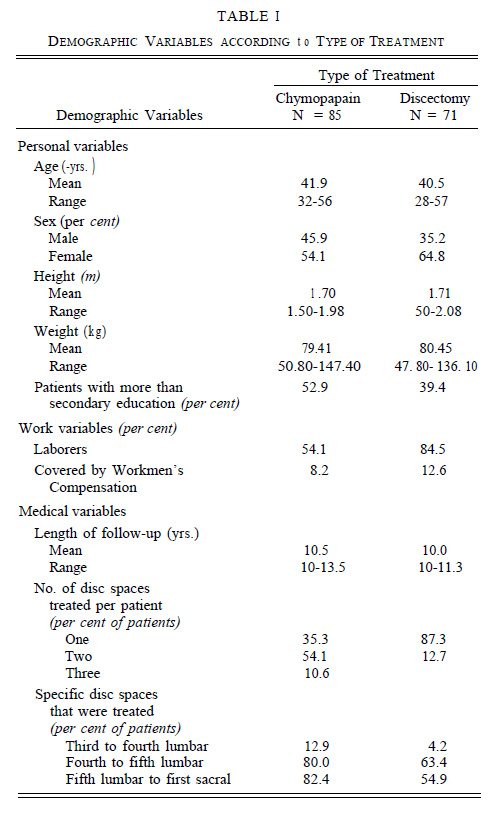
The demographic variables for the chymopapain and discectomy patients are summarized in Table I. The de-mographics were categorized into three distinct types of variable: personal, work, and medical. In general, the chy-mopapain and discectomy groups were remarkably similar with respect to all three categories. Differences in age, height, and weight were unremarkable. More than 50 per cent of both groups were women, with the percentage of women slightly higher in the discectomy group. There were slight differences in the amount of education and in the number of patients who were laborers, indicating that those in the chymopapain group were better educated and, pre-dictably, less likely to be laborers. The patients in the dis-cectomy group were slightly more likely to be covered by Workmen’s Compensation. The two groups were also sim-ilar in terms of the length of the follow-up interval. How-ever, the groups were not well matched as to the number of disc spaces that were treated in each patient or the specific spaces that were treated. The chymopapain patients were more likely to have had two or three disc spaces treated at the same procedure, and the percentages of the chymopapain patients who were treated for lesions at each of the three lower-lumber levels (third to fourth lumbar, fourth to fifth lumbar, and fifth lumbar to first sacral) were higher than the percentages of the discectomy patients so treated (Table I). These differences were not unexpected, given the nature of the experimental protocol used for the chymopapain pa-tients. In the chymopapain group, the levels that were injected were often selected on the basis of positive disco-grams regardless of symptoms, whereas in the discectomy group the levels that were treated were chosen based on symptoms as well as myelographic findings.
Pain-Outcome Measures
Validity studies of the six pain-outcomemeasures were carried out to make sure that they accurately reflected the patients’ condition. The intercorrelations among the six pain-outcome measures are summarized in Table II. The high intercorrelations among these six measures support the notion that these measures did assess related or similar things.
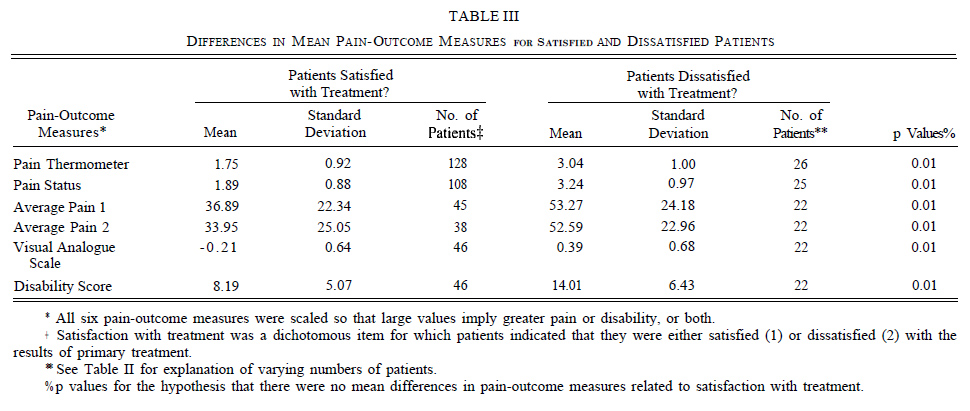
As a second test of validity, patients in the chymopapain and discectomy groups were combined, and a oneway multivariate analysis of variance (MANOVA) was done to assess the relationships between the six pain-outcome measures and the patients’ satisfaction with their treatment (see Appendix). It was postulated that satisfaction with treatment would be highly related to the pain-outcome measures, since patients who were satisfied with their treatment would be likely to have less pain than the less satisfied ones, or alternatively, patients with less pain would be more likely to be satisfied with their treatment than would patients with more pain. The results of the multivariate analysis of variance indicated a strong relationship between satisfaction with treatment and the six pain-outcome measures considered as a group, Wilk’s criterion F 6,53 = 4.00, p < 0.003. Follow-up univariate tests (see Appendix) indicated that for each of the pain-outcome measures, the patients who were satisfied with their treatment reported significantly less pain than the patients who were less satisfied (Table III).
Results of the one-way multivariate analysis of variance to assess the relationships between the six pain-outcome measures and type of treatment (chymopapain compared with open discectomy) showed no significant relationship, Wilk’s criterion F6 54 = 1.18, p < 0.34. Thus, the chymopapain and discectomy groups were not distinguishable on the basis of the pain-outcome measures at the ten-year follow-up.
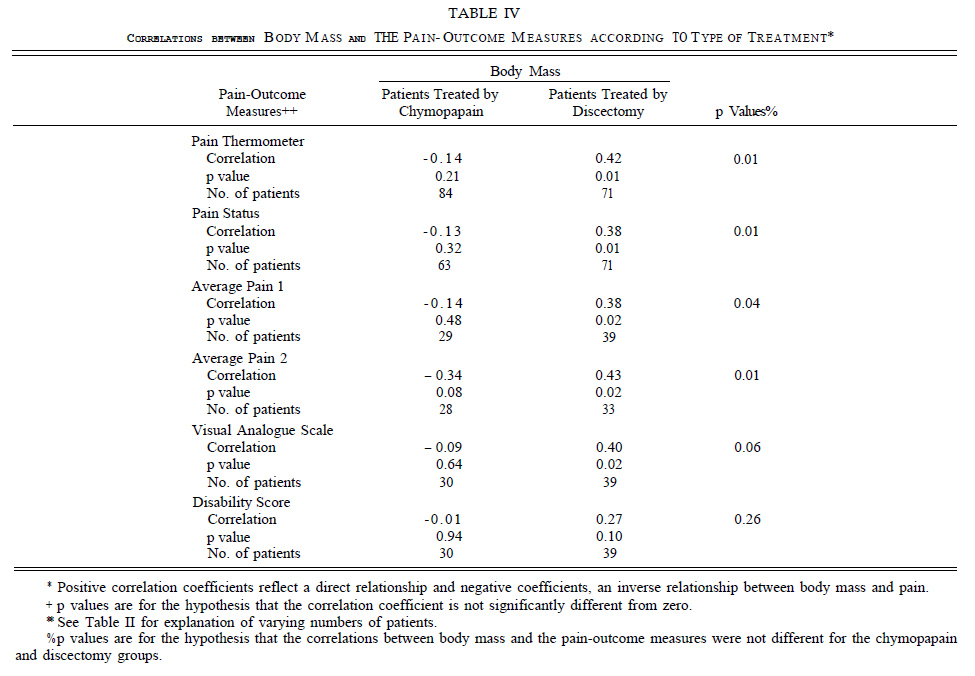
Additional tests were done to determine whether there was any relationship between body mass2 (body weight in kilograms divided by the square of body height in meters – kilograms per square meter) and the pain-outcome measures. These tests were designed to show whether the relationships between body mass and the pain-outcome measures were distinct for the two treatment groups or whether there was an interaction between the type of treatment and body mass reflected in the pain-outcome measures. Results of a multivariate analysis of variance for the overall results showed a trend indicative of some interaction between mode of treatment and body mass (Wilk’s criterion F6.52 = 1.96, p < 0.09). This trend was reflected in five of the six pain-outcome measures. Thus, body mass was a better predictor of pain outcome in the discectomy patients than in the chymopapain patients for five of the six painoutcome measures (Pain Thermometer, Pain Status, Average Pain 1 and 2, and Visual Analogue Scale). However, body mass was not a significant predictor of the disability score for either treatment group.

The correlations between body mass and each painoutcome measure are summarized in Table IV. The differences between the chymopapain and discectomy groups are striking. For the chymopapain group, all of the correlations between body mass and the pain-outcome measures were negative, but none of the correlations was judged to differ significantly from zero. For the discectomy group, on the other hand, all of the correlations were positive and all but one were found to differ from zero by a statistically significant amount. Even though the numbers of subjects for the tests of some of these variables were small (Table IV), the similarities of the results for the pain-outcome measures suggest that the relationship between body mass and pain was different for the chymopapain group than for the discectomy group.
Progress Measures
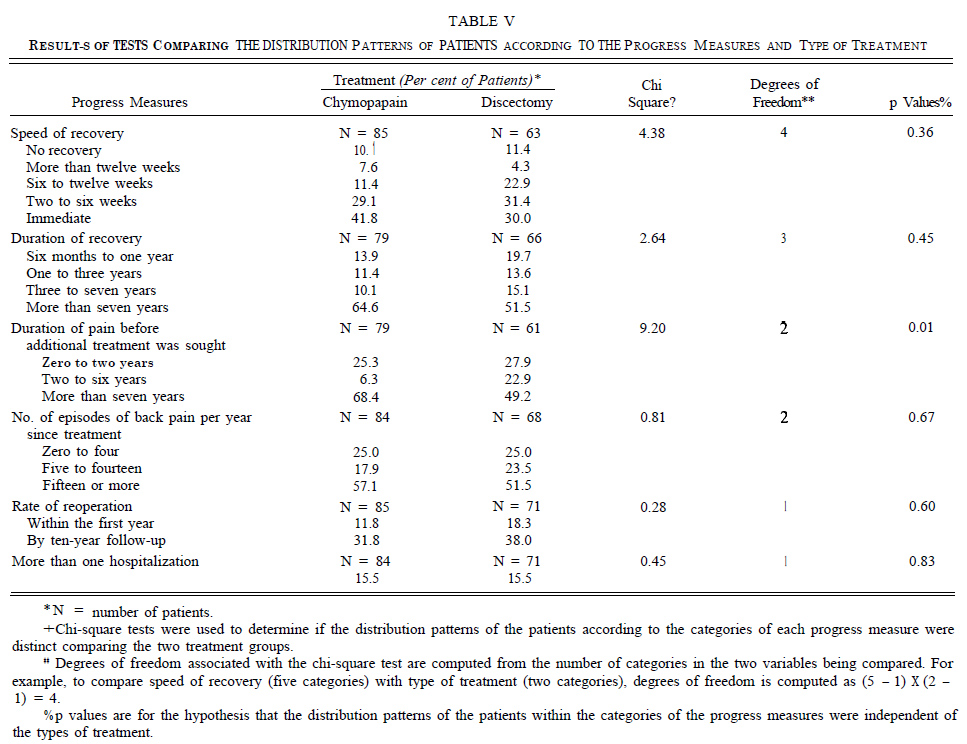
The relationships between the six progress measures and the two types of treatment are summarized in Table V. A statistically significant relationship was evident between the type of treatment and the duration of pain before the patient sought additional treatment because of persistent pain (chi square = 9.2, p < 0.01). Also, as shown by the distribution of patients with respect to this measure, patients in the chymopapain group were more likely than those in the discectomy group to endure pain for a prolonged period. Thus, 68.4 per cent of the chymopapain patients and 49.2 per cent of the discectomy patients endured pain for more than seven years before seeking additional treatment. The chymopapain and discectomy groups did not differ significantly from one another with respect to any of the other five progress measures.
Of particular interest a priori was the relationship between the type of treatment and the incidence of reoperation. Although no statistically significant differences in the incidences of reoperation in the two treatment groups were observed, there was a non-significant trend suggesting that the rates of reoperation at both one and ten years were higher among the discectomy patients. Thus, 18.3 per cent of the discectomy and 11.8 per cent of the chymopapain patients had been reoperated on during the first year after the initial procedure, and 38.0 per cent of the discectomy and 3 1.8 per cent of the chymopapain patients had had additional procedures at the time of the ten-year follow-up.
Other trends shown by the data (Table V) suggested that the chymopapain patients were relieved of pain more quickly (70.9 per cent of the chymopapain and 6 1.4 per cent of the discectomy patients were relieved within six weeks); that their relief was of longer duration (64.6 per cent of the chymopapain and 5 I .5 per cent of the discectomy patients reported no pain for more than seven years); and that they were slightly more likely to have frequent episodes of back pain (in 57.1 per cent of the chymopapain patients, and in 5 1.5 per cent of the discectomy patients, the average number of episodes of back pain each year was more than fifteen).
Work Measures
The relationships between the type of treatment and the work measures are summarized in Table VI. Again, the similarities between the two treatment groups in terms of these measures were more remarkable than the differences. The likelihoods of the patients returning to work and of retaining the same job were quite similar in both treatment groups: 90.4 per cent of the chymopapain and 87.0 per cent of the discectomy patients returned to work, and 75.3 per cent of the chymopapain and 78.9 per cent of the discectomy patients retained the same jobs. The chymopapain patients were slightly more likely to return to work quickly than were the discectomy patients (4 I .8 per cent of the chymopapain and 30.0 per cent of the discectomy patients returned to work within six weeks after treatment). Also of interest, although not readily interpretable, was the finding that of the few patients who did change jobs, the ones in the chymopapain group were much more likely to switch to a job that required no manual labor than were the discectomy patients (63.6 per cent compared with 36.4 per cent). This finding may be related in some measure to a higher level of education in the chymopapain group.
Effect of Time of Returning to Work on Results
As previously described, this effect was analyzed using three composite variables (A, B, and C) based on the time when symptoms were relieved (a progress measure) and the time when the patients returned to work (a work measure). The patients were divided into the three composite-variable groups and then the patients in each of these groups were subdivided on the basis of the time of relief of symptoms and the time of return to work. Finally, the corresponding composite-variable subgroups in the chymopapain and discectomy groups were compared.
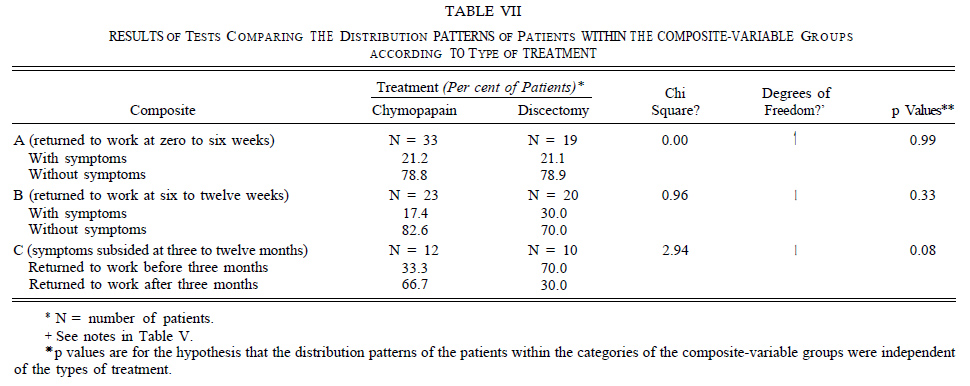
The Composite-A group was comprised of the patients who returned to work zero to six weeks after initial treatment with or without symptoms at the time that they resumed work. The Composite-B group included the patients who returned to work six to twelve weeks after primary treatment, some with and some without residual symptoms at that time. The Composite-C group, on the other hand, was made up of the patients whose symptoms had not subsided until three to twelve months after initial treatment. In this composite-variable group, the patients who had returned to work less than twelve weeks after primary treatment were compared with the ones who had resumed work more than twelve weeks after treatment.
The distributions of the patients according to the three composite-variable groups and the type of treatment are shown in Table VII. Consistent with most of the previous findings, the distributions of patients in the Composite-A? Composite-B, and Composite-C groups were independent of the type of treatment; that is, speed of relief of symptoms in conjunction with speed of returning to work were not related to type of treatment.
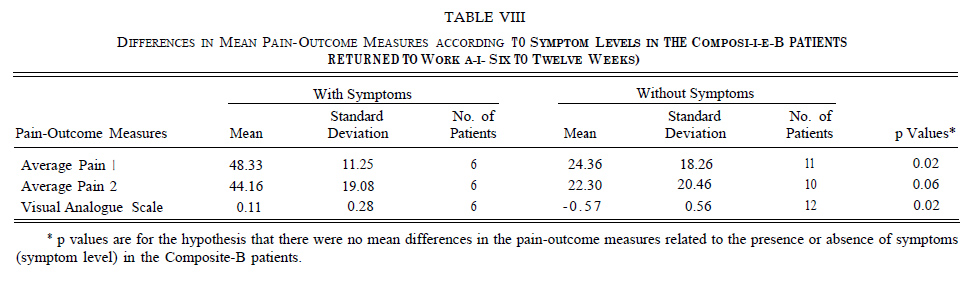
To determine whether the type of treatment and any of the composite variables might be useful in explaining the findings relative to the pain-outcome and progress measures, two-way multivariate analyses of variance were carried out (see Appendix). For the pain-outcome measures, these tests showed no significant over-all interactions between the type of treatment and the three composite variables. Thus, the Wilk’s criteria were: F5 6 = 2.17 (p < 0.21) for Composite A, F6.7 = 0.81 (p < 0.60) for Composite B, and F6.1 = 5.82 (p < 0.3 1) for Composite C. However, for the patients in the Composite-B group (returned to work between six and twelve weeks), there was a significant over-all main effect (see Appendix) indicated by the pain-outcome measures, Wilk’s criterion F6.7 = 4.31 (p < 0.04). The significant pain-outcome findings at follow-up for the Composite-B patients, as determined by univariate analyses, are summarized in Table VIII. The tabulated mean values of the three pain-outcome meaures that were significantly different indicate that the main effects manifested by these measures were in the same direction. Among the Composite-B patients, the ones who were still not well at the time of return to work had significantly more pain or less well-being at the ten-year follow-up than the ones who were well when they returned to work. Although, as already noted, the differences in the results in the Composite-A group were not significant, the differences in the mean values according to type of treatment in this group reflected changes in the same direction as those in the Composite-B group.
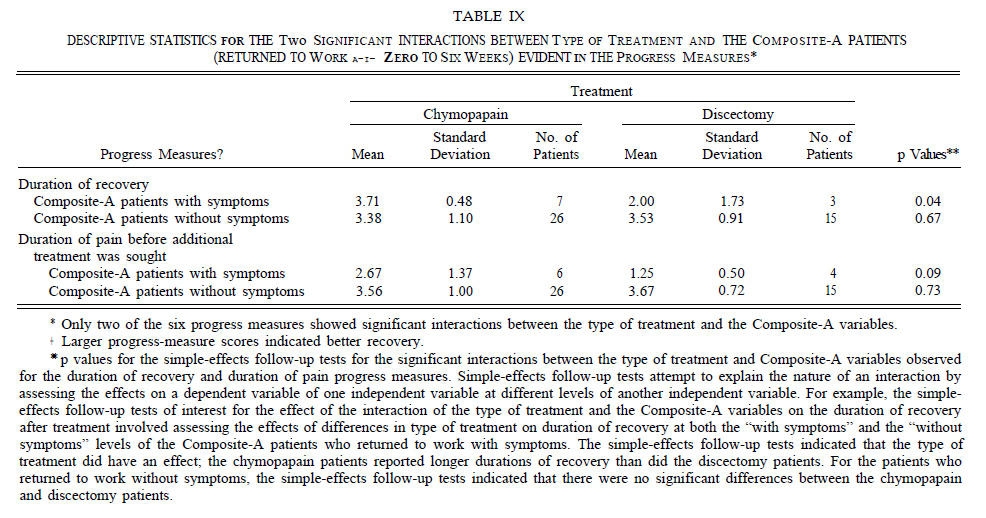
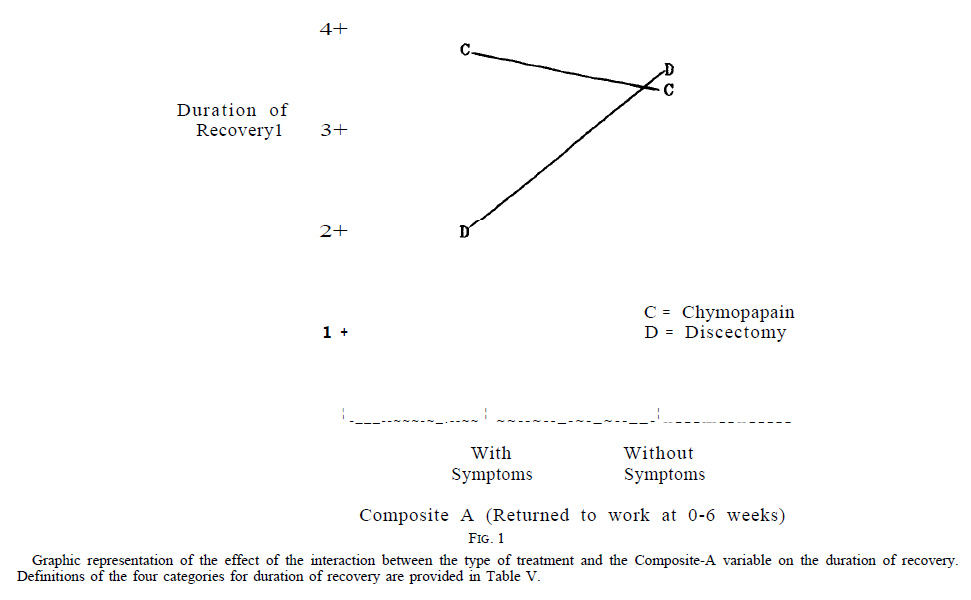
The progress measures, on the other hand, showed that the interactions between the type of treatment and the composite variables were not significant for the Composite-B but were significant for the Composite-A and Composite-C variables: Wilk’s criterion F6,40 = 1.97 (p < 0.10) for Composite A and F6.7 = 5.23 (p < 0.03) for Composite C. In the Composite-A group, the follow-up univariate analyses (see Appendix) indicated that there were significant interactions between type of treatment and this composite variable for two of the six progress measures: the duration of recovery (p < 0.03) and the duration of pain before additional treatment was sought (p < 0.03). The patterns of the means of these two measures indicated that both interactions were of the same form. Follow-up simple-effects tests (see notes in Table IX) indicated that for both of these interactions, the discectomy patients who still had symptoms when they returned to work had significantly poorer results compared with all other patients. These patients had a shorter duration of recovery and were likely to wait a shorter period of time before seeking additional treatment than did the discectomy patients who returned to work without symptoms and all of the chymopapain patients. Descriptive statistics for these analyses are given in Table IX. The patterns of the mean values for the interactions between the type of treatment and the duration of recovery (a progress measure) in the Composite-A group are shown in Figure 1.
In the Composite-C group, the follow-up univariate analyses indicated that the interaction between the type of treatment and this composite variable was marginally significant with respect to only one of the progress measures: duration of pain before additional treatment was sought (p< 0.07). However, there were no data to suggest that progress toward recovery was poorer when patients with per-sistent symptoms returned to work more than twelve weeks after primary treatment. Also, it should be noted that the extremely small number of Composite-C patients (Table VII) made meaningful interpretation difficult.
Satisfaction with Treatment
Finally, we looked for any correlation between the two types of treatment, the patients’ satisfaction with the treatment, and their willingness to have the same treatment again. We found no significant differences: 85.5 percent of the chymopapain patients and 80.3 per cent of the discectomy patients were satisfied with their treatment (chi square = 0.76, p < 0.38), while 79.5 per cent of the chymopapain and 84.3 per cent of the discectomy patients indicated that they would be willing to have the treatment again if need be (chi square = 0.32, p < 0.58). However, we did find significant differences between the two treatment able on the basis of the pain-outcome measures. However, we did find significant differences between the two treatment groups with respect to the patients’ willingness to recommend treatment to friends. Here, 90.3 per cent of the chymopapain and only 7 1.3 per cent of the discectomy patients indicated that they would recommend the treatment to friends (chi square = 9.10, p < 0.01).
Discussion
In this investigation, we used a longitudinal case-study design to analyze the results during a ten-year period in two groups of patients with similar back pain or lower-extremity pain, or both, who had received two different treatments: chymopapain injection or open discectomy. Unfortunately, longitudinal studies of this type have inherent weaknesses. First, retrospective analysis of records in order to develop a study population is often difficult. However, in this study the record-keeping systems at both hospitals minimized these problems. Second, finding patients after ten years and getting them to respond is no small task. Although the over-all return rate of the patients contacted in this study was more than 98 per cent (97 per cent for the chymopapain and 100 per cent for the discectomy patients), we could not locate 29.7 per cent (seventy-six) of the 256 initially iden-tified patients. Third, the use of questionnaires to generate follow-up data has a number of problems. Patients often skip questions, so that the data are incomplete or missing and, perhaps more importantly, patients may randomly or systematically incorrectly recall information concerning the progress of their recovery during a ten-year period. Some patients in this study skipped items in the questionnaire, and there was no way to determine whether all patients were providing accurate information since some responded to certain questions inconsistently. For example, patients might indicate that they had had a second operation during the first year after their initial treatment at one point in the questionnaire and elsewhere indicate that their second pro-cedure was performed two years after the first operation. When such inconsistent reports were noted, these responses were eliminated from subsequent analyses. Finally, studies of this nature are not randomized and, therefore, differences in treatment outcome do not necessarily imply effects of treatment, a point made by the statistical notion that cor-relation does not imply causality. However, in the defense of this type of research, it is important to remember that causality often does result in correlation. Even with these limitations, the results of this study suggest several poten-tially important points.
The questionnaire used in this study was based on six well accepted measures of pain. In addition, validity studies demonstrated that these measures were adequate reflections of the patients’ condition at least to the extent that the six pain-outcome measures were found to be linearly related to each other. The validity hypothesis – that patients who were satisfied with their treatment would report less pain than patients who were dissatisfied with their treatment – was supported. Consistent with the original hypothesis, the chymopapain and discectomy groups were not distinguishable on the basis of the pain-outcome measures. However, in view of the eventual favorable outcomes of patients who were treated non-operatively for a herniated nucleus pulposus, as documented by Weber, a ten-year follow-up may be too long for useful comparisons of outcomes of different treatments.
An additional test assessing the relationships of the type of treatment and of the pain-outcome measures to the body mass (kilograms per square meter) showed a surprising find-ing. Body mass was positively related to the pain-outcome measures at the ten-year follow-up among the discectomy patients but was unrelated to these measures among the chymopapain patients. The reason or reasons for this dif-ference are not clear, but this finding might suggest that chemonucleolysis may be preferable to discectomy for obese patients.
Expected differences in some of the progress measures were observed. Of particular interest a priori was the re-lationship between the type of treatment and the incidence of reoperation. Reports in the literature have shown that following discectomy the average rate of reoperation is ap-proximately 10 per cent (range, zero to 30 per cent)3.20, while the rates after chymopapain injection have been re-ported to be as high as 52 per cent. Although the differences in the incidences of reoperation after the two treatments in this study were not statistically significant, there was a trend indicating higher rates of reoperation at both one and ten years in the discectomy patients. Other trends found in the progress measures suggested that the chymopapain patients recovered more quickly and were relieved of symptoms for longer periods of time, but were more likely to have frequent episodes of back pain. These trends, together with the sig-nificant relationship indicating that chymopapain patients with persistent pain were likely to wait longer before seeking additional treatment, may suggest a potential superiority of chymopapain over discectomy treatment, or alternatively, that the chymopapain group contained more patients with less severe pain compared with those in the discectomy group. This latter interpretation may be supported by the high number of episodes of pain each year in the chymopapain group. This large number would be possible only if the episodes were of short duration. Sim ilarly, the apparent willingness of the chymopapain patients to endure the pain for more than seven years suggested less intense pain. How-ever, this may be due to the fact that the number of patients who worked at heavy labor was less in the chymopapain group than in the discectomy group. Finally, open discec-tomy is quite likely to result in a slightly longer recovery period than the chymopapain procedure. Therefore, close examination of the trends of the progress measures does not provide unequivocal support for any superiority of chymopapain injection over discectomy.
The studies of the relationships between the type of treatment and the work-related measures were exploratory and, therefore, no specific hypotheses were tested. Although the chymopapain and discectomy groups were quite similar with respect to many of these measures, there was a trend indicating that the chymopapain patients returned to work more rapidly than the discectomy patients. However, speed of returning to work in and of itself s not particularly im-portant. The effects of returni ng to work before or after relief of symptoms after initial treatment are of much greater interest.
Three composite variables, which were created by combining information about the time of relief of symptoms after treatment and the speed of return to work, were used to investigate more carefully the effect on the result of the time of return to work. As suggested by most of the previous findi ngs, these composite variables were independent of the type of treatment. Thus, the chymopapa.in and discectomy patients did not differ significantly with respect to the percentage of patients who returned to work with or without symptoms after the initial procedure. However, the composites did provide useful information for the prediction of the long-term effects of return to work with or without symptoms.
Among the patients who returned to work between six and twelve weeks after treatment, those who still had persistent symptoms had significantly greater pain at the ten-year follow-up. A similar pattern of resu lts was observed in the patients who returned to work within six weeks after treatment, with or without persistent symptoms but these trends were notstatistically significant Of particular interest were the patients whohad notbeen relieved at twelve weeks. For them, there were no significant differences between the patients who did and did not return to work at twelve weeks. Thus, returning to work at twelve weeks may not have deleterious long-term effects even if symptoms persist at the time of resuming work. For patients who returned to work within six weeks after treatment, there was a relation between the type of treatment, the time when symptoms were relieved, and the duration of pain relief. The discectomy patients who returned to work with symptoms had a significantly shorter duration of pain relief than the other discectomy patients. In the chymopapain patients, however, the duration of pain relief was not related to the time when pain was relieved. Thus, for discectomy patients more thanfor chymopapain patients, the duration of pain relief after treatment may have been more crucially related to the speed of return to work and the time when symptoms were relieved after treatment.
The pain-outcome measures at the ten-year follow-up were not significantlyrelated to the type of treatment. How-ever, the patients whowere satisfied with treatment had less pain than the ones who were less satisfied. Also, the patients who returned to work within six to twelve weeks after initial treatment, before they were relieved of symptoms, had significantly more pain than the patients who returned to work during this same period but were free of symptoms at the time when they resumed work. Using the progress measures, the type of treatment was found to be.related to the duration of pain (after the initial treatment) before additional treatment was sought. Compared with the discectomy patients, the chymopapain patients endured the pain significantly longer before seeking additional treatment. Several trends in the data suggested slight superiority of chymopapain injection over discectomy but these findings, especially in light of the constraints of the study, must be considered preliminary. The interaction of the type of treatment and of the time after treatment when symptoms were relieved was found to predict the duration of symptomatic relief, and here again the findings favored chymopapain treatment. Thus, although the type of treatment in and of itself was not a predictor of the result, the type of treatment in conjunction with other rel evant variables, such as body mass and du-ration of painbefore seeking addi tional treatment, provided information that did help to predict findings that are important in clinical practice In this retrospective study, surgical techniques varied according to the preferences of the physicians and thus were not controlled. The results might be different today, with the availability of newer, less intrusive surgical techniques. To test this hypothesis would require a controlled prospec-trial wtive ith one surgeon using the same techniques each time. Due to the known anatomical and pathological variability of patients, such a study would be difficult to perform.
Finally, correlating the patients’ sati sfaction ten years after treatment with the type of treatment showed the following results. Among the discectomy patients, those who stated that they would have the treatment again outnumbered those who were satisfied with their treatment. The discectomy patients were also relatively reluctant to recomment this treatment to a friend. Among the chymopapain patients, on the other hand, those who stated that they would recommend the treatment to a friend outnumbered those who were satisfied with the treatment, and even fewer would have the treatment again themselves. In light of these findings, one must wonder about the quality of friendship among the patients who were treated with chymopapain.
Conclusions
- After a ten-year follow-up, the results of discectomy and chymopapain injection were not distinguishable on the basis of six well established pain-outcome measures (Table III).
- Trends that were evident in the data suggested that the discectomy patients had had a higher incidence of repeat procedures at both one and ten years after the original treat-ment.
- In the absence of clinical improvement after primary treatment, returning to work within the first twelve weeks after treatment may be ill advised.
- If the patients return to work after twelve weeks, the long-term outcome is apparently not affected by whether or not they had symptoms at the time of return.
Appendix
Multivariate analysis of variance is the general case of analysis of variance. Analysis of variance is a statistical technique that is often used to assess differences in mean values of a dependent variable at different levels of categorical independent variables. When there is more than one dependent variable, a multiple analysis of variance is often the appropriate initial or over-all test of significance. In this test, each dependent variable is not considered separately but instead a composite of the dependent measures is created; mean values of this composite for each level of the categorical independent variables are computed, and the differences between these composite means are tested. If this over-all test (usually Wilk’s criterion) is significant, then follow-up tests assessing the effectsof the independent variables on each individual dependent variable, often called univariate follow-up tests, can be done. However, if the result of the over-all multivariate analysis of variance is not significant and univariate follow-ups are done anyway, the nominal or observed error rate (p value) will be an under-estimation of the true error rate. To illustrate this, suppose that univariate follow-up analyses of variance are done despite a non-significant over-all multivariate analysis of variance and one of the dependent variables Y is found to be significantly related to an independent variable X (p = 0.04). This main effect of X on Y indicates that there are differences in the mean values of Y at the various levels of X. Since the over-all multivariate analysis of variance was not significant, it is probable that the 0.04 level of significance for the main effect of X on Y underestimated the true probability of error. Therefore, it would probably be incorrect to attribute mean differences in the dependent variable Y to the effects of the independent variable X, and any generalization about the ability of the independent variable to affect the dependent variable based on this result might be wrong. In summary, when an experimental design attempts to assess the effects of an independent variable or variables on more than one dependent variable, failure to use multivariate techniques that explicitly deal with the error-rate problems associated with multiple dependent variables can lead to consistent overestimation of the effects of the independent variables.
* No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. No funds were received in support of this study.
+ Department of Orthopaedic Surgery, University of Iowa Hospitals and Clinics, Iowa City, Iowa 52242.
** Department of Orthopaedics, Rush Presbyterian-X Luke’s Medical Center, Chicago, Illinois 60611.
References
- BAXTER-TRAVENOL: Brand of Chymopapain Injection, Investigational New Drug 1004. Travenol Laboratories, Incorporated, Deerfield, Illinois, 1963- 1975.
- BRAY, G. A. [editor]: Obesity in America. Department of Health, Education and Welfare Publication (NIA) 79-359, Washington, D.C., National Institutes of Health, 1979.
- CAUCHOIX, J. ; FICAT, C. ; and GIRARD, B. : Repeat Surgery after Disc Excision. Spine, 3: 256-259, 1978.
- CRAWSHAW, C.; FRAZER, A. M.; MERRIAM, W. F.; MULHOLLAND, R. C.; and WEBB, J. K.: A Comparison of Surgery and Chemonucleolysis in the Treatment of Sciatica. A Prospective Randomized Trial. Spine, 9: 195- 198, 1984.
- GARRON, D. C., and LEAVITT, FRANK: Chronic Low Back Pain and Depression. J. Clin. Psychol., 39: 486-493, 1983.
- HAKELIUS, ANDERS: Prognosis in Sciatica. A Clinical Follow-up of Surgical and Non-Surgical Treatment. Acta Orthop. Scandinavica, Supplementurn 129, 1979.
- JACKSON, R. K.: The Long-Term Effects of Wide Laminectomy for Lumbar Disc Excision. A Review of 130 Patients. J. Bone and Joint Surg., 53-B(4): 609-6 16, 197 1.
- JAVID, M. J.: Treatment of Herniated Lumbar Disc Syndrome with Chymopapain. J. Am. Med. Assn., 243: 2043-2048, 1980.
- Leavitt, F.: Detecting Psychological Disturbance using Verbal Pain Measurement. The Back Pain Classification Scale. In Pain Measurement and Assessment, pp. 79-84. Edited by Ronald Melzack. New York, Raven Press. 1983.
- LEAVITT, FRANK; GARRON, D. C.; WHISLER, W. W.; and C. M.: A Comparison of Patients Treated by Chymopapain and Laminectomy for Low Back Pain using a Multidimensional Pain Scale. Clin. Orthop., 146: 136- 143, 1980.
- LEAVITT, FRANK; GARRON, D. C.; WHISLER, W. W.; and SHEINKOP, M. B.: Affective Sensory Dimensions of Back Pain. Pain, 4: 273-281, 1978.
- MCCULLOCH, J. A.: Chemonucleolysis. Experience with 2000 Cases. Clin. Orthop., 146: 128-135, 1980.
- MILLION, R.; HALL, W.; HAAVIK NILSEN, K.; BAKER, R. D.; and JAYSON, M. I. V.: Assessment of the Progress of the Back-Pain Patient. Spine, 7: 204-212, 1982.
- MIXTER, W. J., and BARR , J. S.: Rupture of the Intervertebral Disc with Involvement of the Spinal Canal. New England J. Med., 211: 2 10-2 15, 1934.
- NASHOLD, B. S., JR., and HRUBEC, ZDENEK [editors]: Lumbar Disc Disease. A Twenty-Year Clinical Follow-up Study. St. Louis, C. V. Mosby, 1971.
- RAVICHANDRAN, G., and MULHOLLAND, R. C.: Chymopapain Chemonucleolysis. A Preliminary Report. Spine, 5: 380-384, 1980.
- ROLAND, MARTIN, and MORRIS, RICHARD: A Study of the Natural History of Back Pain. Part I: Development of a Reliable and Sensitive Measure of Disability in Low-Back Pain. Spine, 8: 141-144, 1983.
- ROLAND, MARTIN, and MORRIS, RICHARD: A Study of the Natural History of Low-Back Pain. Part II. Development of Guidelines for Trials of Treatment in Primary Care. Spine, 8: 145-150, 1983.
- SMITH, LYMAN: Enzyme Dissolution of the Nucleus Pulposus in Humans. J. Am. Med. Assn., 187: 137-140, 1964.
- SPANGFORT, E. V. : The Lumbar Disc Hemiation. A Computer-Aided Analysis of 2,504 Operations. Acta Orthop. Scandinavica, Supplementurn 142, 1972.
- SUSSMAN, B. J.: Inadequacies and Hazards of Chymopapain Injections as Treatment for Intervertebral Disc Disease. Neurosurg . , 42: 389-396, 1975.
- WEBER, HENRIK: Lumbar Disc Hemiation. A Controlled, Prospective Study with Ten Years of Observation. Spine, 8: 131-140, 1983.
BY J. WEINSTEIN, D.O.+, K. F. SPRATT, M.A.+, IOWA CITY, IOWA, T. MCNEILL, M.D.*, AND W. HEJNA, M.D.+, CHICAGO, ILLINOIS
From the Department of Orthopaedic Surgery, University of Iowa Hospitals and Clinics, Iowa City and the Department of Orthopaedics, Rush Presbyterian-St. Luke’s Medical Center, Chicago
[Reprinted from The Journal of Bone and Joing Surgery Vol. 68-A, No. 1. pp. 43-54. January 1986] Copyrighted 1986 by The Journal of Bone and Joint Surgery, inc. Printed in U.S.A.





 Our patients can receive MRI imaging onsite at both our Louisville and New Albany Clinics.
Our patients can receive MRI imaging onsite at both our Louisville and New Albany Clinics. Providing the latest advances in orthopedic surgery is our specialty.
Providing the latest advances in orthopedic surgery is our specialty. We take a unique, multidisciplinary approach to pain management.
We take a unique, multidisciplinary approach to pain management. Our physical therapists use advanced techniques to help restore strength and mobility.
Our physical therapists use advanced techniques to help restore strength and mobility.  We provide comprehensive, conservative care for a wide variety of foot and ankle conditions.
We provide comprehensive, conservative care for a wide variety of foot and ankle conditions. We offer same- and next-day care to patients with acute injuries.
We offer same- and next-day care to patients with acute injuries. Get back in the game with help from our sports medicine specialists.
Get back in the game with help from our sports medicine specialists.  Our centers are equipped with a state-of-the-art digital X-ray machine.
Our centers are equipped with a state-of-the-art digital X-ray machine.