



Efficacy of Electroacupuncture and TENS in the Rehabilitation of Chronic Low Back Pain Patients 1
Aug 22, 2019Fifty-four patients treated in a 3-week inpatient rehabilitation program were randomly assigned to and accepted treatment with electroacupuncture (n = 17) TENS (low intensity transcutaneous nerve stimulation, n = 18) and TENS deadbattery (placebo, n = 18). Outcome measures included estimates of pain (on a Visual Analogue Scale) and disability by both physician and patient, physical measures of trunk strength and spine range of motion, as well as the patient’s perceptions of the relative contribution of the education, exercise training, and the electrical stimulation. Analyses of variance were utilized to determine effects of treatment (electroacupuncture, TENS, placebo) across time (admission, discharge, and return) for the outcome measures. There were no significant differences between treatment groups with respect to their overall rehabilitation. All 3 treatment groups ranked the contribution of the education as being greater than the electrical stimulation. However, the electroacupuncture group consistently demonstrated greater improvement on the outcome measures than the other treatment groups. For the visual analogue scale measure of average pain, there was a statistical trend at the return visit suggesting that the acupuncture group was experiencing less pain.
- Supported in part by NIHR Grants 23P59176 and GOO8435055
- Address reprint requests and correspondence to: Thomas R. Lehmann, M.D., Associate Professor, Department of Orthopaedic Surgery, University of Iowa, 1197 Carver Pavilion, Iowa City, IA 52242, U.S.A
Introduction
Low back pain is one of the most common ailments in Western Society: 80% of all adults have significant back pain during their lifetime [15,36]. Of the working population, 26% will experience low back pain annually and 8% will experience a low back disability [14]. Over a lifetime, 28% of an industrial population will be at least temporarily disabled by back pain [43]. Three percent of all low back cases in industry will be disabled longer than 3 months [4]. Low back pain is also one of the most costly ailments to society in terms of medical expenses and lost worktime [19]. Leavitt et al. [21] found that these costs are skewed with 25% of all low back pain disability claimants accounting for 87% of the costs. Therefore, proper management of chronic low back pain patients (pain duration greater than 3 months) from the industrial population is especially important because they account for an overwhelming majority of costs. The majority of chronic low back pain patients do not have a diagnosable condition for which a specific treatment, such as lumbar surgery, can be applied [20]. These patients should be considered for a formal rehabilitation program.
Traditional rehabilitation programs have employed non-surgical modalities derived from multiple disciplines: therapeutic exercise, progressive physical activity, postural training, occupational therapy, drug management, and relaxation techniques. However, only 33-42% of industrial patients return to work following rehabilitation [3,37,52]. The relative contributions of each of the multiple modalities is unknown. The authors have considered a strategy to systematically test these contributions so that rehabilitation efforts can be optimized. In the proposed model, all subjects receive a core curriculum which consists of education and exercise training. Subjects then are randomly assigned to either active or control treatment groups. Active treatment groups receive the core curriculum as well as that treatment modality which might potentially enhance the rehabilitation effort. Control treatment groups receive only the core curriculum.
Electrical stimulation for control of pain is commonly employed in multidisciplinary rehabilitation programs. There are several uncontrolled reports on the value of conventional high transcutaneous electrical nerve stimulation (TENS) in various pain syndromes [2,5,8,38-40,42,45]. There is disagreement about subthreshold TENS. Long et al. [26] found that after 3 consecutive days of stimulation, subthreshold TENS was no more effective than a unit without a battery. However, our own empiric experience was that subthreshold TENS was quite effective. Therefore, subthreshold TENS was selected as one of the active treatments to be tested.
Acupuncture-like stimulation has been shown to have a slower induction time [9] and to be inhibited by the morphine antagonist naloxone [44] in contrast to TENS. Several controlled studies support the efficacy of high intensity TENS (acupuncture-like), electroacupuncture, and manual rotation acupuncture. Therefore, electroacupuncture was chosen as an additional active modality to be tested.
The study was undertaken (1) to determine the utility of the proposed model, and (2) to specifically determine if electrical stimulation for the control of pain has a measurable effect on the rehabilitation of chronically disabled low back pain patients. It is hoped that this report will stimulate new ideas about ways to determine the optimum curriculum for a multidisciplinary pain management program.
Methods
Patients with chronic disabling low back pain are screened in the University of Iowa Orthopaedic Clinic. After reviewing the clinical history, physical examination, and radiographic findings, patients who are considered candidates for lumbar surgery are excluded. Patients who have had low back pain for less than 3 months and patients with the following diagnoses are also excluded from consideration: pregnancy, osteomyelitis of spine, discitis, tumor, ankylosing spondylitis, vertebral fractures, and structural scoliosis. Of the remaining patients who demonstrate at least minimal levels of motivation and in whom the level of disability would warrant the expense of inpatient treatment, applications are given for admission. Not all patients apply.
Fifty-four patients meeting the above criteria were admitted to the Inpatient Rehabilitation Program from 3/3/80 to 5/10/82. At admission, these patients were randomly assigned to I of 3 treatment groups. Some of the patients had recent lumbar surgery, and others no prior lumbar surgery. Because it was felt that this variable could influence the outcome, the randomization scheme controlled for whether the patient had prior lumbar surgery. In conducting the random assignment to treatment, patients were assigned to I of 3 blocks: (A) block 1 – surgery performed less than 6 months prior to admission; (B) block 2 – surgery performed between 6 and 12 months prior to admission; (C) block 3 – surgery performed more than 12 months prior to admission or no prior history of lumbar surgery. The patients within each block were then randomly assigned to the TENS, TENS with dead battery, or electroacupuncture treatment. Patients could withdraw at any time from the electrical stimulation protocol. One patient refused to accept the assigned treatment, leaving 53 subjects in the study.
When the assigned treatment was either TENS or TENS dead battery, the patients had the electrodes attached and were stimulated with a live battery. For both treatments, the intensity of stimulation was then reduced to the point that the patient could not feel the stimulation. At that point, the assigned battery (active or dead) was placed in the unit, and the unit was placed in a plastic case. Patients were told not to open the case or tamper with the controls on the unit. The physician and physical therapist applying the TENS were blind to the type of battery used. The nurse investigator was the only one who knew which patient was receiving active or dead battery treatment. The nurse would test the batteries regularly to insure that the patients were receiving either an active or dead battery treatment as assigned.
TENS and TENS dead battery treatments were offered daily except weekends during the 3-week program. A physical therapist experienced in the application of TENS stimulated the patients at a pulse width of 25O/sec, frequency of 60 Hz, and subthreshold intensity. Points of stimulation were over the center of pain. In patients with significant leg pain, stimulation was also performed over the related nerve trunk.
Electroacupuncture treatments were offered on a twice-weekly schedule. A certified acupuncturist experienced in its application stimulated the patients with needles. The stimulus was a biphasic wave at a frequency of 2-4 Hz and was increased to the patient’s level of tolerance. Visible muscle contractions usually occurred. Stimulation loci were along the inner and outer bladder meridian if the pain was lateral (sciatica). Hoku point and additional points were usually stimulated according to the patient’s pattern of pains. Other aches and pains were often treated concomitantly to the low back pain treatment.
At admission, patients completed an objective clinical history questionnaire. A detailed physical examination by the orthopedic resident was recorded on a physical examination data sheet. Physical measurements of trunk strength and spine range of motion by trained investigators were recorded. A patient’s periodic record, physician’s periodic record, and trunk strength and range of motion measurements were performed at admission, discharge, and at a 6-month return visit.
Trunk strength was measured 5 times in the seated position for flexion and extension. The results were then averaged and recorded in kilograms. To control for the effect of sex on trunk strength, the strength score for female patients was multiplied by 1.61 for extension and 1.76 for flexion [22]. Spine range of motion was measured with a gravity goniometer between the first thoracic and first sacral vertebrae in both flexion and extension and recorded in degrees.
On the patient’s periodic record, the patient rated (1) the degree of peak pain experienced since the last assessment, and (2) the general level of pain on an average day. Both of these assessments were recorded on a 10 cm ungraduated line, the ends of which represented very severe pain and no pain, respectively (Visual Analogue Scale). The point on the line where the patient estimated his pain was measured, and 1-15 points were awarded for freedom from pain on each scale (more points meant less pain). Patients estimated their degree of disability by choosing I of 5 responses: (1) no disability (10 points), (2) able to work full time but at lower level (8 points), (3) able to work part-time at usual level (6 points), (4) able to work only part-time but at lower level (4 points), or (5) not able to work at all (0 points). In addition, the patient reported on his/her ability to perform 15 activities of daily living. One point was awarded for each activity the patient perceived he/she was capable of performing.
On the physician’s periodic record, the physician estimated the level of pain he would expect for the patient on an average day. This item was identical to the patient’s estimate discussed above except that 1-10 points were assigned for freedom from pain (more points meant less pain). The physician also estimated the degree of impairment that the patient had on a multiple choice item. One to 5 points were awarded for the following responses: no impairment = 5; mild, but should not affect most activities = 4; moderate, cannot perform some strenuous activities = 3; only light activities = 2; and severely limited = 1. The physician questioned the patient about medication usage and awarded points according to the level of analgesics taken in an average day: non-narcotic, occasional use (10 points); non-narcotic, regular use (8 points); minor narcotic, regular use (4 points); major narcotic, occasional use (2 points); major narcotic, regular use (0 points).
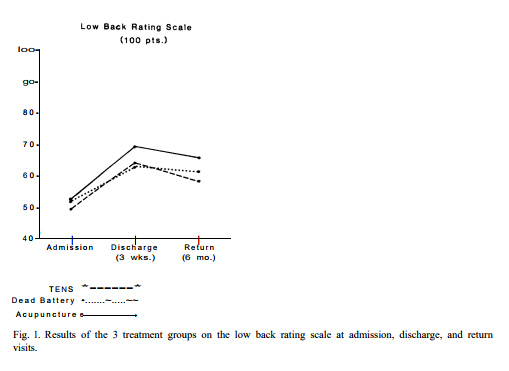
The above 8 items (excluding the peak pain measure) were summed to derive a total Low Back Rating Scale Score (0-100 points). All of the variables were scaled so that greater points mean better function, less pain, and less disability. The mean scores for each treatment group on the Total Rating Scale were compared to test the hypothesis that patients receiving electroacupuncture and live TENS would show greater overall improvement than the dead-battery placebo group.
In addition to the Rating Scale components, each patient indicated the degree of benefit received from the overall program at the discharge and return visit. Patients were asked to rate the contribution that each component of the program made to their overall benefit by responding to the following questions: (a) How much has the educational program helped your overall treatment result? (b) How much has the exercise program helped your overall treatment result? and (c) How much has the electrotherapy helped your overall treatment result? On each question they could choose 1 of 5 responses: (1) worse, (2) no major change, (3) small, but important improvement, (4) great benefit, (5) very great benefit. Return to work data were collected by telephone, mailed questionnaires, and medical records of clinic visits.
Results
Descriptive information is first presented that indicates the characteristics of the sample and considers the effect of subject attrition. The results of analyses of variance testing for differences between treatment groups across time on the 10 outcome measures (8 individual items from the Low Back Rating Scale, the Total Rating Scale Score, and Visual Analogue Score of peak pain) are then presented. In general, the analyses fail to demonstrate a significant benefit of electrical stimulation to the overall rehabilitation effort, but they do demonstrate a reduction in the patient’s perception of pain for the electroacupuncture group. An overall observation was, that although the acupuncture treated group mean socres were not significantly greater on the other outcome measures, this group consistently demonstrated superior mean scores at discharge and return than the other 2 groups. Therefore, an analysis of how each group ranked with respect to each other for all outcome measures is also presented. Finally, to explore the value of the electrical stimulation from a different approach, an analysis of the patients’ perceptions of the relative contribution of education, exercise, and electrotherapy to the overall benefit is presented.
Descriptive information
Of the 53 subjects in the study, 17 were female. Ages ranged from 25 to 55 years, with a mean of 40. All had low back pain for greater than 6 months, and only I was working at admission to the program. Fifty-eight percent were receiving worker’s compensation benefits, and another 20% of the patients were receiving long-term disability payments from their company or union. Approximately half had applied for social security. Fifty-seven percent had retained a lawyer for matters related to their low back disability. Forty-eight percent had prior lumbar surgery, for a mean number of 1.2 back operations. The medical records indicated a tentative diagnosis of: (a) low back pain of unknown etiology, n = 26; (b) lumbar motion segment instability, n = 8; (c) lumbar spinal stenosis, n = 8; (d) herniated nucleus pulposus with radiculopathy, n = 5; (e) discogenic pain without radiculopathy, n = 4; and (f) functional low back pain, n = 2.
Seventeen patients received electroacupuncture, 18 patients subthreshold TENS (transcutaneous electrical nerve stimulation), and 18 patients TENS with a dead battery. There have been no treatment complications. All patients also took part in a comprehensive multidisciplinary educational program and twice daily exercise training sessions. Formal psychotherapy, relaxation training, biofeedback and hypnosis were not included in the treatment.
Of 17 patients in the acupuncture group, 4 dropped out after only 1 treatment. In the TENS and TENS dead-battery groups, 4 of 18 and 3 of 18 dropped out after 3 treatments, respectively. The dropout rate was not significantly different across the treatment groups, xz = 0.29, P = 0.87. In the subsequent analyses, dropouts from the treatment groups were included.
A second source of attrition was the failure of patients to return for the 6-month follow-up visit. Five of the acupuncture and 4 of the TENS patients did not return, whereas all the patients in the TENS dead-battery group did return. Thus, at return, there were 12 patients in the acupuncture, 14 patients in the TENS, and 18 patients in the TENS dead-battery groups. This dropout rate was considered differential across the treatment groups, xi = 5.89, P < 0.06. Although failure to return did not hinder the assessment of treatment effects from admission to discharge, an overall picture of treatment effectiveness over the more extended time period was more difficult to assess since failure to return may have been related to treatment effectiveness.
Mean admission and discharge scores for patients who did not return at the 6-month follow-up were compared to assess possible effects of this attrition. No overall attrition effects were observed on any of the criteria. However, a treatment group by attrition interaction was observed for the trunk strength measures at both admission and discharge and for the patient’s perception of contribution to the overall benefit from the exercise program. The form of all 3 interactions was the same. In each case, the 4 non-returning patients in the TENS group scored higher (i.e., had greater trunk strength and rated exercise of greater benefit) than the other groups.
Twenty-one of the 53 subjects have not returned to any gainful activity (TENS, n = 6; dead battery, n = 8; acupuncture, n = 7). Three subjects returned to normal work in the home (TENS, n = 2; acupuncture, n = 1). Three subjects returned to full-time student activities (TENS, n = 1; acupuncture, n = 2). Twenty-six subjects returned to full-time gainful employment (TENS, n = 9; dead battery, n = 10; acupuncture, n = 7). However, 5 have been laid-off (TENS, n = 2; dead battery, n = 2; acupuncture, n = 1) and 4 have been terminated because their back impairment, kept them from working (TENS, n = 1; dead battery, n = 2; acupuncture, n = 1). Excluding these latter 4 subjects, 28 of 53 (53%) have been able to return to and maintain gainful activity. The rate of return to gainful activity did not vary across the treatment groups (xz = 0.2936, P < 0.87).
Comparisons of the treatment groups
The 10 outcome measures (8 individual items from the Low Back Rating Scale, the Total Rating Scale Score, and Visual Analogue Score of peak pain) were analyzed by conducting a series of 3 X 3 (3 treatment groups measured at 3 times) repeated measures of analyses of variance. With the exception of the Visual Analogue Scale measure of average pain, there were no significant treatment by time interactions.
Without regard for treatment group, mean scores on all 10 outcome measures demonstrated highly significant gains from admission to discharge (P value ranged from 0.0117 to 0.0001). Similarly, there were significant long-term gains from admission to return for all outcome measures, with the exception of medications and peak pain scores (P values ranged from 0.045 to 0.0001). In general, the mean scores for each group demonstrated improvement from admission to discharge, but regression from discharge to return.
This typical pattern was demonstrated for the Total Rating Scale Score (Fig. l), where the treatment main effect and treatment by time interactions were not statistically significant (P = 0.60 and P = 0.57, respectively), but the time main effect was significant ( F2 9l . = 49.67, P = 0.0001). Thus, the 3 treatment groups were not significantly different from each other at admission, discharge, or return Considering each treatment over time, there was significant improvement from admission to discharge for the TENS, TENS dead-battery, and acupuncture groups ( P < 0.0001, P < 0.002, P < 0.0001, respectively), and a non-significant regression from discharge to return (P = 0.10, P = 0.67, P = 0.41, respectively). Overall, all 3 groups showed long-term benefits as measured from admission to return (P = 0.01, P = 0.001, P = 0.004, respectively).
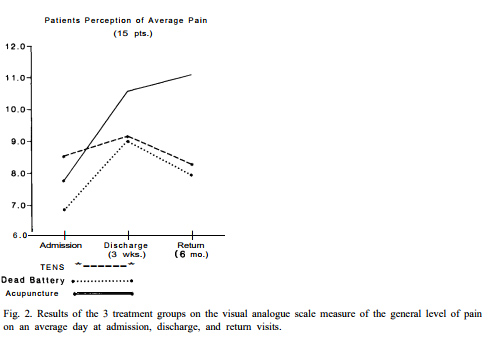
On the average pain measure, there was a statistically significant treatment by time interaction ( F4, 9l = 2.99, P < 0.03) (Fig. 2). Tests of simple effects of the interaction demonstrated that at admission the mean pain scores were not significantly different between the 3 treatment groups (TENS dead-battery = 8.55, TENS = 6.83, acupuncture = 7.76; F2 5. = 1.50, P < 0.24). Considering each treatment over time, the TENS group experienced a non-significant gain followed by a non-significant loss. Over time, the dead-battery group showed significant improvement from admission to discharge (P = 0.03) and a non-significant loss from discharge to return. The acupuncture group significantly improved from admission to discharge (P = 0.005) and showed a non-significant gain from discharge to return. Whereas the TENS and TENS dead-battery groups did not demonstrate significant long-term gains as measured from admission to return (P = 0.50 and P = 0.23, respectively), the acupuncture group did (P = 0.0008). Although the acupuncture group demonstrated less average pain with a higher mean score at discharge, the differences across treatment groups were not significantly different (TENS dead-battery = 9.00, TENS = 9.16, acupuncture = 10.59; F2 5. = 1.66, P < 0.20). However, at the return visit the acupuncture mean average pain score indicated significantly less pain compared to the dead-battery and active TENS groups (dead-battery = 7.94, n = 18; TENS = 8.28, n = 14; acupuncture = 11.08, n = 12; F2 4l = 3.57, P = 0.04) *.
For each of the 10 outcome measures at admission and the 11 outcome measures at discharge and return (including the assessment of overall benefit), the treatment groups were ranked according to whether their mean scores were high, middle, or low. Thus, the treatment group with the best mean score (least pain and/or greatest function) would be ranked high and the treatment group with the worst mean score (greatest pain and least function) would be ranked low. At admission, chi-square analysis of a 3 X 3 design (3 treatments and 3 classifications) indicated no significant differences between the groups (xi = 2.25, P = 0.69). At discharge, the acupuncture mean scores ranked highest on 10 of the 11 measures and middle on 1 of the 11 (xi= 33.24, P < 0.0001). At return, the acupuncture mean scores ranked highest on 6 of the 11 measures and middle on 5 of the 11 (xi = 9.94, P < 0.05).
The mean scores for the 5-point scale rating the contribution to overall benefit made by the education, exercise, and electrotherapy components of the rehabilitation program demonstrated that, for each of the 3 treatment groups at both discharge and return, education was considered to have contributed more to the overall benefit than the electrotherapy (P < 0.05). Mean scores for the educational contribution ranged from 3.56 to 3.94 (3 = small contribution, 4 = great contribution). Mean scores for the electrotherapeutic contribution ranged from 2.41 to 3.00 (2 = no contribution, 3 = small contribution). In general, patients in all treatment groups at both times ranked the contributions from best to least as education, exercise, and electrotherapy.
Discussion
The original intent of the study was to determine the contribution that electrical stimulation for the control of pain would make to the rehabilitation of inpatients with disabling low back pain. The rehabilitation program has been established as a model to test the relative contribution of the various modalities utilized in a multidisciplinary inpatient chronic pain program. The hypothesis tested was that greater improvement in the low back rating scale could be demonstrated for groups receiving active electrical stimulation than groups receiving dead-battery TENS. Although there were no significant differences in improvement between treatment groups, the acupuncture group demonstrated slightly better results. All 3 groups demonstrated highly significant short-term (admission-discharge) and long-term (admission-return) improvements on the Total Rating Scale measure (P < 0.01). Additional data supporting this finding were that there were no differences between the return to work rates across the treatment groups. The patients perceived that the educational component contributed the most to their overall benefit and found the electrical stimulation least helpful. These results in no way, however, imply that there was no benefit to the patients from their electrical stimulation. The results do imply that the patients received significant overall benefit from the total program and that we could not detect that the electrical stimulation added significantly to that benefit.
* This significance level was not adjusted for the effects of multiple comparisons. When adjusted for these effects, the significance was reduced to the 0.10 level, which still suggests a trend in the data.
In fact, the electroacupuncture group consistently ranked the highest across all outcome measures, suggesting that this form of electrical stimulation was efficacious. It is impossible to know what impact the effect of many subjects dropping out of electroacupuncture had on these results. Coan et al. [7] reported that patients receiving a minimum of 8 acupuncture treatments report less pain at a 40-week follow-up than patients who drop out after only 1 or 2 treatments and discussed the effects of attrition on efficacy. Of additional concern is the fact that the acupuncture group had the largest number of subjects who did not return for the 6-month assessment (5 of 17). However, assessment of the data from the discharge visit did not demonstrate significant differences between those who ultimately did and did not return on the average pain measure.
One concern of the authors was that the differences on the average pain measure between treatment groups were not statistically significant at the discharge assessment, although there was a trend toward significance at the return assessment. Intuitively, it was expected that the differences should be maximized at the conclusion of treatment rather than at the 6-month return visit. One explanation of this finding is proposed. It is generally accepted that an inactive TENS unit may have a placebo benefit of short duration. Therefore, at conclusion of treatment the placebo benefit makes it difficult to demonstrate the effect of an otherwise efficacious treatment such as electroacupuncture. However, with the placebo benefit wearing off over time, the true differences would be best demonstrated at a return visit.
An additional concern is that the acupuncture treatment is not being compared to a blinded control. Other studies have either refused to use a placebo control group on the grounds that this is unethical [7], used a dummy stimulator as we have [28,33,48], simulated acupuncture treatments by stimulating with less than therapeutic intensities (nail-prick [17], low electrical intensity with needles [29,35], or simulated acupuncture but used non-acupuncture points [6,17]). Melzack et al. [34] have used a different treatment all together (massage) rather than a sham acupuncture treatment as a control. They suggest that sham treatments cannot be blind controls because patients will always be able to detect the difference between active and non-active stimulation. Patients in this study were aware of whether they were assigned to a TENS-type group or the electroacupuncture group. Inasmuch as the acupuncturist is an experienced pain therapist, he may have had a therapeutic effect over and above that of the electroacupuncture treatment alone. Also, since the electroacupuncture treatment is quite uncomfortable (muscles are stimulated to tolerance), it is possible that this treatment has a greater placebo benefit. However, ordinarily one expects placebo benefits to last less than 6 months [1,10,26,48].
Although there are several controlled studies which support the efficacy of high intensity acupuncture-like TENS [6,13,16,33,34], subthreshold TENS has been thought to be no better than placebo by Long and Hagfors [27]. This study was also unable to detect any differences between active subthreshold TENS and dead-battery TENS.
Several additional limitations of this study should be noted. As indicated above, a substantial proportion of the patients in all 3 treatment conditions did not complete the full regimen. This may have reduced the efficacy of the treatments. A related limitation in terms of evaluating the effectiveness of these treatments concerns the nature of this patient population, the majority of which had work-related injuries. Successful treatment of similar chronic low back patients is very difficult, with low rates of rehabilitation (approximately 40%) routinely found in clinical studies [3,52]. An additional limitation is related to the presence of subjects who invalidly report pain within the sample. In a previous report [23], we were able to demonstrate that patients with nonorganic physical findings biased the overall results of the study. Other authors have concluded that ‘functional’ or ‘psychogenic’ patients may be recalcitrant to electrical stimulation for the control of pain [25,27,31]. Given the above limitations, substantial improvement under any form of treatment regimen is therefore unlikely to be found. Thus, small levels of improvement, as was found in this study, may perhaps be the best one can expect from even a very effective treatment, given the nature of the patient population.
Ideally, future studies would establish admission criteria that are strict enough that only relevant treatment-sensitive subjects would be enrolled so that the ‘true’ efficacy of treatment can be determined. However, the results of such a study would not be generalizable to the ‘average’ disabled low back pain patient referred to multidisciplinary pain treatment centers.
In terms of assessing the outcome of the interventions, several limitations of the study are apparent. First, our follow-up data were not very extensive, being limited to a 3-6-month interval. We are continuing to follow these patients and will eventually be able to report long-term data concerning the effectiveness of these treatments.
A final problem concerns the outcome measures themselves. Although we have tried to gather data that indicate improvement in patients from a variety of sources, it is difficult to know which measures should be weighted more heavily in drawing final conclusions. Since electrical stimulation as utilized here is a pain-relief modality, perhaps its efficacy should be judged solely on its ability to relieve pain rather than its ability to affect disability. This limitation raises the issue of whether the research model employed here has utility. In the proposed model, the contributions that individual modalities make over and above a basic rehabilitation program of patient education and exercise are tested. However, as demonstrated by the significant improvement of patients regardless of treatment group on all outcome measures, it is possible that no efficacious treatment could demonstrate a contribution of sufficient magnitude to be detected. This may especially be true in view of the small sample sizes usually available for studies of this type.
However, it is possible that patients disabled by a chronic low back condition are not suffering so much from pain but rather from a behavioral disability. Whereas physical disability is essentially constant after initial healing in the acute phase following injury, psychological disability steadily increases over time [ 3]. Significant psychological problems have been found in chronic low back patients by many authors [3,12,30,46]. A contingency approach to rehabilitation involves the systematic elimination of pain behaviors as suggested by Fordyce et al. [ll]. Psychological interventions such as operant conditioning [18,24,50,51], relaxation training [24,50], and cognitive behavioral methods [32,47,49], have been utilized on chronic pain patients with success. Roberts and Reinhardt [41] reported a 77% success rate (return to normal lifestyle) in chronic low back patients using an operant approach. Perhaps the research model proposed here would prove successful if psychological interventions were tested as the active intervention.
The ability of electroacupuncture and subthreshold transcutaneous electrical stimulation to enhance the rehabilitation of chronic low back patients undergoing a multidisciplinary inpatient treatment program has been tested. With the methods employed, neither electrical stimulation modality was shown to affect the patients’ rehabilitation. Electroacupuncture demonstrated the ability to reduce some pain reports. Subthreshold TENS was no more effective than a dead-battery control. The limitations of the study are discussed with the hope that future studies will be able to avoid some of these limitations through improved designs.
References
- Andersson, S.A., Pain control by sensory stimulation. In: J.J. Bonica et al. (Eds.), Advances in Pain Research and Therapy, Vol. 3, Raven Press, New York, 1979, pp. 569-585.
- Augustinsson, L.E., Bohlin, P., Bundsen, P. et al., Pain relief during delivery by transcutaneous electrical nerve stimulation, Pain, 4 (1977) 59-65.
- Beals, R.K. and Hickman, N.W., Industrial injuries of the back and extremities. Comprehensive evaluation – an aid in prognosis and management: a study of one hundred and eighty patients, J. Bone Jt Surg., 54A (1972) 1593-1611.
- Berquist-Ullman, M. and Larsson, U., Acute low back pain in industry. A controlled prospective study with reference to therapy and confounding factors, Acta orthop. scand., Suppl. 170 (1977) 9-117.
- Burton, C., Transcutaneous electrical nerve stimulation to relieve pain, Postgrad. Med., 59 (1976) 105-108.
- Chapman, C.R., Wilson, M.E. and Gehrig, J.D., Comparative effects of acupuncture and transcutaneous stimulation on the perception of painful dental stimuli, Pain, 2 (1976) 265-283.
- Coan, R.M., Wong, G., Ku, S.L., Chan, Y.C., Wang, L., Ozer, F.T. and Coan, P.L., The acupuncture treatment of low back pain: a raandomized controlled study, Amer. J. Chin. Med., 8 (1980) 181-189.
- Dougherty, R.J., TENS – an alternative to drugs in the treatment of chronic pain. Presented at the First General Scientific Meeting of the American Pain Society, San Diego, CA, September 9-12, 1979.
- Eriksson, M. and Sjolund, B., Acupuncture-like electroanalgesia in TNS-resistant chronic pain. In: Y. Zotterman (Ed.), Sensory Functions of the Skin, Oxford University Press, New York, 1976, pp. 575-581.
- Evans, F.J., The placebo response in pain reduction, Adv. Neurol., 4 (1974) 289-296.
- Fordyce, W., Fowler, R., Lehmann, J., DeLateur, B., Sand, P. and Trieschmann, R., Operant conditioning in the treatment of chronic pain, Arch. phys. Med. Rehab., 54 (1973) 399-408.
- Forrest, A.J. and Wolkind, S-N., Masked depression in men with low back pain, Rheum. Rehab., 13 (1974) 148-153.
- Fox, E.J. and Melzack, R., Comparison of transcutaneous electrical stimulation and acupuncture in the treatment of chronic pain. In: J.J. Bonica and D. Albe-Fessard (Eds.), Advances in Pain Research and Therapy, Raven Press, New York, 1976, pp. 797-801.
- Gyntelberg, F., One year incidence of low back pain among male residents of Copenhagen aged 40-59, Dan. med. Bull., 21 (1974) 30-36.
- Horal, J., The clinical appearance of low back disorders in the city of Gothenburg, Sweden, Acta orthop. scand., Suppl. 118 (1969) 1-109.
- Jeans, M.E., Relief of chronic pain by brief, intense transcutaneous electrical stimulation – a double-blind study, Adv. Pain Res. Ther., 3 (1979) 601-606.
- Junnila, S.Y.T., Acupuncture therapy for chronic pain. A randomized comparison between acupuncture and pseudo-acupuncture with minimal peripheral stimulus, Amer. J. Acupunct., 10 (1982) 259-262.
- Keefe, F.J., Behavioral assessment and treatment of chronic pain: current status and future directions, J. consult. clin. Psychol., 50 (1982) 896-911.
- Kelsey, J.L. and White, III, A.A., Epidemiology and impact of low back pain, Spine, 5 (1980) 133-142.
- Kelsey, J.L., White, A.A., Pastides, H. and Bisbee, Jr., G.E., The impact of musculoskeletal disorders on the population of the United States, J. Bone Jt Surg., 6lA (1979) 959-964.
- Leavitt, S.S., Johnston, I.L. and Beyer, R.D., The process of recovery: patterns in industrial back injury. Part 4. Mapping the health care process, Indust. Med., 41 (1972) 5-9.
- Lehmann, T.R., Brand, R.A. and Gorman,T.W.O., A low-back rating scale, Spine, 8 (1983) 308-315.
- Lehmann, T.R., Russell, D.W. and Spratt, K.F., The impact of patients with nonorganic physical findings on a controlled trial of transcutaneous electrical nerve stimulation and electroacupuncture, Spine, 8 (1983) 625-634.
- Linton, S.J., A critical review of behavioral treatments for chronic benign pain other than headache, Brit. J. clin. Psychol., 21 (1982) 321-337.
- Loeser, J.D., Black, R.G. and Christman, A., Relief of pain by transcutaneous stimulation, J. Neurosurg., 42 (1975) 308-314.
- Long, D.M., Campbell, J.N. and Gucer, G., Transcutaneous electrical stimulation for relief of chronic pain, Adv. Pain Res. Ther., 3 (1979) 593-599.
- Long, D.M. and Hagfors, N., Electrical stimulation in the nervous system: the current status of electrical stimulation of the nervous system for relief of pain, Pain, 1 (1975) 109-123.
- MacDonald, A.J.R., Macrae, K.D., Master, B.R. and Rubin, A.P., Superficial acupuncture in the relief of chronic low back pain. A placebo-controlled randomised trial, Ann. roy. Coll. Surg. Engl., 65 (1983) 44-46.
- Mao, W., Ghia, J.N., Scott, D.S., Duncan, G.H. and Gregg, J.M., High versus low intensity acupuncture analgesia for treatment of chronic pain: effects on platelet serotonin, Pain, 8 (1980) 331-342.
- McCreary, C. and Jamison, K., Consultation-Liaison Psychiatry, Grune and Stratton, New York, 1975.
- McCreary, C., Turner, J. and Dawson E., Differences between functional versus organic low back pain patients, Pain, 4 (1977) 73-78.
- Meichenbaum, D. and Turk, D.C., The cognitive-behavioral management of anxiety, anger, and pain. In: P.0. Davidson (Ed.), The Behavioral Management of Anxiety, Depression, and Pain, Brunner/Mazel, New York, 1976.
- Melzack, R., Prolonged relief of pain by brief, intense transcutaneous somatic stimulation, Pain, 1 (1975) 357-373.
- Melzack, R., Vetere, P. and Finch, L., Transcutaneous electrical nerve stimulation for low back pain. A comparison of TENS and massage for pain and range of motion, Phys. Ther., 63 (1983) 489-493.
- Mendelson, G., Selwood, T.S., Kranz, H., Loh, T.S., Kidson, M.A. and Scott, D.S., Acupuncture treatment of chronic back pain. A double-blind placebo-controlled trial, Amer. J. Med., 74 (1983) 49-55.
- Nachemson, A., The lumbar spine – an orthopaedic challenge, Spine, 1 (1976) 59-71.
- Newman, RI., Seres, J.L., Yospe, L.P. and Garlington, B., Multidisciplinary treatment of chronic pain: long-term follow-up of low back pain patients, Pain, 4 (1978) 283-292.
- Procacci, P., Zoppi, M. and Maresca, M., Transcutaneous electrical stimulation in low back pain: a critical evaluation, Acupunct. electro-ther. Res., 7 (1982) 1-6.
- Rausch, D., TENS – is it acupuncture without needles?, R. Home Care, August-September (1981) 81-85.
- Richardson, R.R., Arbit, J. and Zagar, R., Evaluation of transcutaneous electrical neurostimulation, J. psychosom. Res., 24 (1980) 79-83.
- Roberts, A.H. and Reinhardt, L., The behavior management of chronic pain: long-term follow-up with comparison groups, Pain, 8 (1980) 151-162.
- Rosenberg, M., Curtis, L. and Bourke, D.L., Transcutaneous electrical nerve stimulation for the relief of postoperative pain, Pain, 5 (1978) 129-133.
- Rowe, M.L., Low back disability in industry. Updated position, J. occup. Med., 12 (1971) 476-478.
- Sjolund, B. and Eriksson, M., Electra-acupuncture and endogenous morphines, Lancet, ii (1976) 1085.
- Solomon, R.A., Viernstein, MC. and Long, D.M., Reduction of postoperative pain and narcotic use by transcutaneous electrical nerve stimulation, Surgery, 87 (1980) 142-146.
- Sternbach, R.A., Wolf, S.R., Murphy, R.W. and Akeson, W.H., Aspects of chronic low back pain, Psychosomatics, 14 (1973) 52-56.
- Tan, S., Cognitive and cognitive-behavioral methods for pain control: a selective review, Pain, 12 (1982) 201-228.
- Thorsteinsson, G., Stonnington, H.H., Stillwell, G.K. and Elveback, L.R., The placebo effect of transcutaneous electrical stimulation, Pain, 5 (1978) 31-41.
- Turk, D.C., Meichenbaum, D. and Genest, M., Pain and Behavioral Medicine: a Cognitive-Behavioral Perspective, Guilford Press, New York, 1983.
- Turner, J.A. and Chapman, C.R., Psychological interventions for chronic pain: a critical review. I. Relaxation training and biofeedback, Pain, 12 (1982) 1-21.
- Turner, J.A. and Chapman, C.R., Psychological interventions for chronic pain: a critical review. II. Operative conditioning, hypnosis, and cognitive-behavioral therapy, Pain, 12 (1982) 23-46.
- White, A.W.M., Low back pain in men receiving workmen’s compensation, Canad. med. Ass. J., 95 (1966) 50-56.
Daniel W. Russell,, Kevin F. Spratt, Hutha Colby, Y. King Liu, Mary Lou Fairchild and Stanley Christensen





 Our patients can receive MRI imaging onsite at both our Louisville and New Albany Clinics.
Our patients can receive MRI imaging onsite at both our Louisville and New Albany Clinics. Providing the latest advances in orthopedic surgery is our specialty.
Providing the latest advances in orthopedic surgery is our specialty. We take a unique, multidisciplinary approach to pain management.
We take a unique, multidisciplinary approach to pain management. Our physical therapists use advanced techniques to help restore strength and mobility.
Our physical therapists use advanced techniques to help restore strength and mobility.  We provide comprehensive, conservative care for a wide variety of foot and ankle conditions.
We provide comprehensive, conservative care for a wide variety of foot and ankle conditions. We offer same- and next-day care to patients with acute injuries.
We offer same- and next-day care to patients with acute injuries. Get back in the game with help from our sports medicine specialists.
Get back in the game with help from our sports medicine specialists.  Our centers are equipped with a state-of-the-art digital X-ray machine.
Our centers are equipped with a state-of-the-art digital X-ray machine.